Inhaler Technique Guide: How to Use Every Asthma Inhaler Correctly
Your inhaler is only as effective as your technique. Studies consistently show that up to 90% of asthma patients make at least one critical error when using their inhaler -- and poor technique is one of the most common reasons asthma remains uncontrolled despite appropriate medication prescriptions. When an inhaler is used incorrectly, as little as 10% of the medication may actually reach the airways where it is needed.
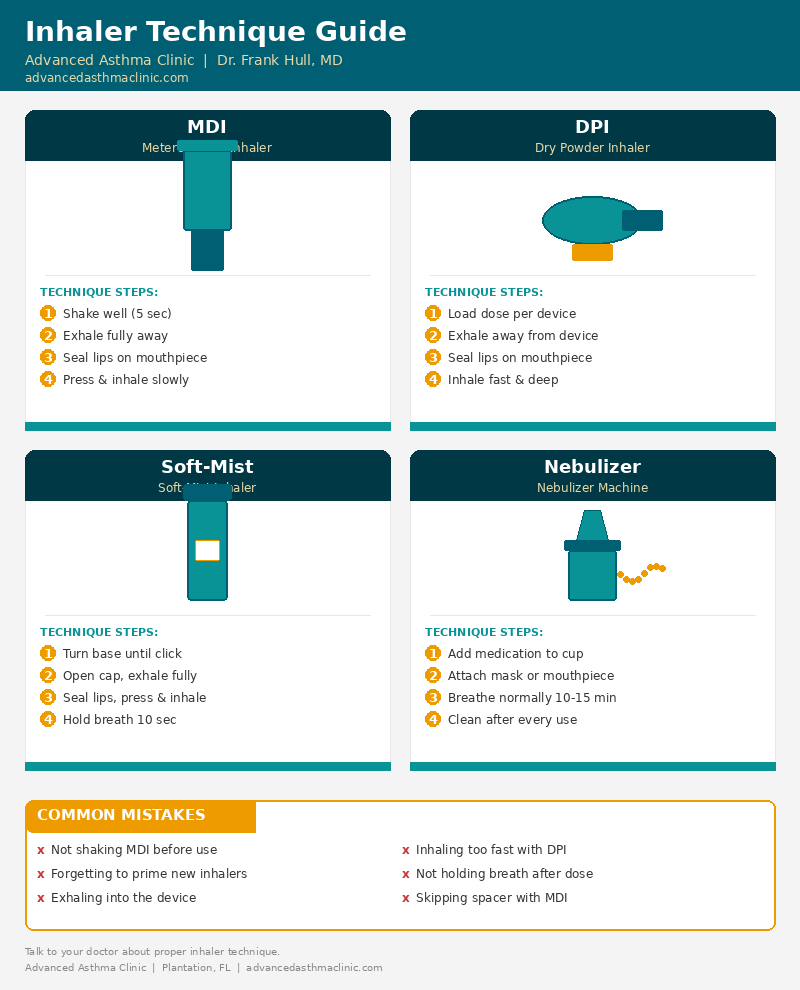
Understanding the differences between inhaler devices, mastering the correct technique for each, and avoiding common mistakes can dramatically improve your asthma control. This guide covers every major inhaler type prescribed for asthma management.
Metered-Dose Inhalers (MDIs)
The metered-dose inhaler is the most commonly prescribed inhaler device worldwide. It uses a pressurized canister to deliver a precise, pre-measured dose of medication as a fine aerosol mist. Common MDI medications include albuterol (rescue inhaler), fluticasone, beclomethasone, and combination inhalers.
Correct MDI Technique (Without Spacer)
- Shake the inhaler vigorously for 5 seconds. The medication is suspended in propellant and must be mixed before each use.
- Remove the cap and hold the inhaler upright with your index finger on top and thumb on the bottom.
- Breathe out fully away from the inhaler -- exhale until your lungs feel empty.
- Place the mouthpiece between your teeth and close your lips around it to form a tight seal.
- Begin breathing in slowly and deeply through your mouth. As you start to inhale, press down firmly on the canister once to release one puff.
- Continue inhaling slowly and steadily for 3-5 seconds until your lungs are completely full.
- Hold your breath for 10 seconds (or as long as comfortable) to allow the medication to settle into your airways.
- Breathe out slowly through your nose or pursed lips.
- Wait 30-60 seconds before taking a second puff if prescribed.
Priming: If your MDI is new or has not been used for several days, prime it by releasing 1-4 test sprays into the air (check your specific medication's instructions) before your first dose.
Common MDI Mistakes
- Not shaking before use -- delivers inconsistent doses and potentially pure propellant without medication.
- Poor coordination -- pressing the canister before or after starting to inhale, so the medication hits the back of the throat instead of reaching the lungs.
- Inhaling too fast -- high-speed inhalation causes medication to impact the throat and mouth rather than penetrating into the lower airways.
- Not holding breath afterward -- exhaling immediately causes much of the medication to be exhaled before it can deposit in the airways.
- Spraying multiple puffs in one breath -- only one actuation per inhalation; multiple puffs overwhelm airflow and waste medication.
- Forgetting to rinse -- for inhaled corticosteroids, always rinse your mouth and spit after use to prevent oral thrush (candidiasis) and hoarseness.
Why Spacers Make a Significant Difference
A spacer (also called a valved holding chamber) is a tube or chamber that attaches to your MDI mouthpiece. It is one of the simplest and most effective ways to improve inhaler drug delivery. Medical guidelines recommend spacer use with all MDI-delivered corticosteroids and for patients who have difficulty with hand-breath coordination.
How Spacers Work
When you press the MDI canister, the medication sprays into the spacer chamber at high velocity -- around 60 miles per hour. The spacer slows down these fast-moving particles, allows the propellant to evaporate, and holds the medication suspended in the chamber for several seconds. This gives you time to inhale without needing perfect coordination. The result: 40-60% more medication reaches your lungs compared to using an MDI alone.
Using an MDI with a Spacer
- Shake the inhaler and attach it to the spacer.
- Breathe out fully away from the spacer.
- Place the spacer mouthpiece between your teeth and seal your lips around it.
- Press the canister once to release medication into the spacer.
- Breathe in slowly and deeply over 3-5 seconds. If you hear a whistling sound, you are breathing in too fast -- slow down.
- Hold your breath for 10 seconds.
- If prescribed a second puff, wait 30-60 seconds and repeat the entire process.
Spacers are particularly important for children, elderly patients, and anyone taking inhaled corticosteroids -- they significantly reduce the risk of oral side effects.
Dry Powder Inhalers (DPIs)
Dry powder inhalers deliver medication as a fine, dry powder rather than an aerosol spray. Unlike MDIs, DPIs are breath-activated -- your inhalation force disperses the powder into particles small enough to reach the lower airways. Common DPI devices include Diskus (Advair, Flovent), Ellipta (Breo, Trelegy), Turbuhaler (Symbicort), and HandiHaler (Spiriva).
Correct DPI Technique
- Load the dose according to your device type -- slide the lever, twist the base, or open the cap (each DPI has a specific loading mechanism).
- Do NOT shake a dry powder inhaler. Unlike MDIs, shaking can cause powder to fall out of the dosing chamber.
- Hold the inhaler level or in the correct position for your device (check the patient leaflet -- some must be held horizontally, others upright).
- Breathe out fully away from the inhaler -- never exhale into the DPI, as moisture from your breath can clump the powder.
- Seal your lips around the mouthpiece and breathe in quickly and deeply -- a fast, forceful inhalation is essential for DPIs to disperse the powder properly.
- Hold your breath for 10 seconds.
- Breathe out slowly away from the device.
Critical difference from MDIs: DPIs require the opposite breathing pattern. While MDIs need slow, steady inhalation, DPIs need a quick, deep, forceful breath to generate enough airflow (typically 30-60 liters per minute) to break up the powder into respirable particles.
Common DPI Mistakes
- Breathing in too slowly -- insufficient inspiratory flow means the powder does not disperse into fine particles and deposits in the throat.
- Exhaling into the device -- moisture clumps the powder and can block the dose.
- Not holding level during loading -- powder can spill from the dosing chamber before inhalation.
- Storing in humid environments -- keep DPIs dry and away from bathroom humidity.
- Not checking the dose counter -- some DPIs continue to "click" even when empty, giving a false sense that medication was delivered.
Patients who cannot generate a strong enough breath -- such as during a severe asthma attack, very young children, or elderly patients with reduced lung capacity -- may be better served by an MDI with spacer or a nebulizer.
Soft-Mist Inhalers (SMIs)
The soft-mist inhaler (most commonly the Respimat device, used for Spiriva Respimat and Stiolto) delivers medication as a slow-moving, fine mist that lasts longer than an MDI spray. This makes coordination easier and increases lung deposition compared to a standard MDI.
Correct SMI Technique
- Turn the clear base a half turn until it clicks (this loads the dose).
- Open the cap fully until it snaps into place.
- Breathe out slowly and fully away from the inhaler.
- Close your lips around the mouthpiece without covering the air vents.
- Breathe in slowly and deeply through your mouth while pressing the dose-release button.
- Hold your breath for 10 seconds or as long as comfortable.
- Close the cap after use.
The soft-mist inhaler produces a mist that travels at about 10% of the speed of an MDI spray, giving you more time to inhale and improving medication delivery to the lungs. Like MDIs, slow and steady inhalation works best.
Nebulizers
A nebulizer converts liquid medication into a continuous fine mist that you breathe in through a mouthpiece or face mask over 5-15 minutes. Nebulizers are commonly used for patients who cannot use handheld inhalers effectively -- including young children, elderly patients, patients during severe exacerbations, and patients on medications only available in liquid form.
Correct Nebulizer Technique
- Wash your hands before assembling the nebulizer.
- Measure the medication and place it in the nebulizer cup. Use pre-measured unit-dose vials when available.
- Connect the tubing from the compressor to the nebulizer cup, and attach the mouthpiece or mask.
- Sit upright in a comfortable position.
- Turn on the compressor and check that a fine mist is visible.
- Breathe normally through your mouth with the mouthpiece between your teeth (or mask over nose and mouth). Take a slow, deep breath every few minutes to maximize deep lung delivery.
- Continue until the nebulizer begins sputtering and no more mist is produced (typically 5-15 minutes depending on the medication volume).
- Clean the nebulizer cup and mouthpiece after every use with warm soapy water, rinse thoroughly, and air-dry on a clean towel.
Nebulizer Maintenance
Proper nebulizer hygiene is essential to prevent bacterial contamination and ensure consistent medication delivery. Disinfect nebulizer parts at least once per week by soaking in a vinegar-water solution (1 part white vinegar to 3 parts water) for 20 minutes, then rinsing and air-drying. Replace nebulizer cups, tubing, and masks according to the manufacturer's schedule -- typically every 3-6 months.
Device Selection: Which Inhaler Is Right for You?
The best inhaler device depends on several patient-specific factors. Your physician considers the following when selecting a device:
- Age: Children under 5 typically use an MDI with spacer and face mask or a nebulizer. Older children and adults can use MDIs, DPIs, or SMIs based on preference and ability.
- Inspiratory flow: Patients who cannot generate a strong enough breath (measured by peak inspiratory flow testing) may not effectively use DPIs.
- Coordination ability: Patients with difficulty coordinating the press-and-breathe maneuver benefit from spacers, breath-activated devices, or nebulizers.
- Dexterity: Patients with arthritis or limited hand strength may find certain devices easier to actuate than others.
- Medication availability: Not all medications come in all device types -- biologic therapies for severe asthma, for example, are delivered by injection rather than inhalation.
- Portability needs: MDIs and DPIs are highly portable; nebulizers require a power source (though portable battery-operated nebulizers are available).
- Patient preference: Adherence improves when patients are comfortable and confident with their device.
Technique Assessment and Coaching
Research demonstrates that even patients who have used inhalers for years develop technique errors over time. Regular technique reassessment -- at every office visit, ideally -- catches errors before they compromise asthma control. If your asthma symptoms have worsened or your rescue inhaler use has increased, poor technique should be considered before changing medications.
At the Advanced Asthma Clinic, Dr. Frank Hull and the clinical team assess inhaler technique as a routine part of every asthma visit. Technique coaching is especially important when:
- Starting a new inhaler device for the first time
- Switching between device types (e.g., from MDI to DPI)
- Asthma control has declined despite consistent medication use
- Lung function testing shows results that do not match expected improvement
- Patients report side effects such as oral thrush, hoarseness, or throat irritation from inhaled corticosteroids
Tips for Getting the Most from Your Inhaler
- Always rinse your mouth after using inhaled corticosteroids -- rinse, gargle, and spit to prevent oral thrush and hoarseness.
- Track your dose counter. Replace your inhaler before it runs out. Do not rely on floating the canister in water -- this method is unreliable.
- Keep a rescue inhaler accessible at all times. Your asthma action plan should specify when and how to use it.
- Store inhalers properly. Keep MDIs at room temperature (cold temperatures reduce output). Keep DPIs dry. Keep all inhalers out of direct sunlight and away from extreme heat.
- Clean your devices regularly. A clogged MDI actuator can reduce output by up to 25% and alter spray characteristics.
- Use one technique for one device type. If you use both an MDI and a DPI, consciously switch your breathing pattern -- slow for MDI, fast for DPI.
- Ask your doctor to watch your technique at every visit, even if you have been using inhalers for years.
Frequently Asked Questions
How do I know if I am using my inhaler correctly?
Key signs of correct technique include: no medication taste on your tongue or throat (it should reach your lungs, not your mouth), the dose counter advances properly, you do not cough immediately after inhaling, and your symptoms improve after use. Your doctor or respiratory therapist can assess your technique and provide coaching during an office visit.
Should I use a spacer with my inhaler?
A spacer is recommended for all metered-dose inhalers (MDIs), especially for inhaled corticosteroids. Spacers improve medication delivery to the lungs by 40-60%, reduce medication depositing in the mouth and throat, decrease the risk of oral thrush, and eliminate the need for precise hand-breath coordination.
What is the difference between an MDI and a DPI?
A metered-dose inhaler (MDI) uses a pressurized canister to spray a measured dose as a fine mist -- requiring slow, steady inhalation. A dry powder inhaler (DPI) delivers medication as a dry powder that requires a fast, forceful inhalation. They require opposite breathing techniques: slow and steady for MDIs, quick and deep for DPIs.
How often should I clean my inhaler?
MDI mouthpieces should be cleaned weekly by removing the canister, rinsing the plastic actuator under warm water, and air-drying completely. DPIs should never be washed with water -- wipe the mouthpiece with a dry cloth. Nebulizer cups and masks should be cleaned after every use and disinfected weekly.
Expert Inhaler Coaching in Plantation, FL
Proper inhaler technique is one of the most impactful, lowest-cost interventions in asthma management. At the Advanced Asthma Clinic, Dr. Frank Hull provides comprehensive personalized asthma care that includes hands-on inhaler technique assessment, device selection tailored to your needs, and ongoing coaching to ensure you are getting the maximum benefit from every dose.
For patients with severe asthma that remains uncontrolled despite proper technique and medication adherence, advanced options including biologic therapies and clinical trial programs may be available. Financial assistance through the Better Breathing Grant program can help reduce the cost of care.
Better technique means better breathing. Call 954-522-7226 to schedule a consultation, or contact us online.
This content is for educational purposes and does not replace professional medical advice. Always consult your physician before making changes to your asthma treatment plan.